Surgeon Paves the Way for Non-Fusion Correction of Scoliosis
https://reports.mountsinai.org/article/ortho2021-02-mount-sinai-surgeon-paves-the-way-for-non-fusion-correction-of
Mount Sinai orthopedic surgeon Baron S. Lonner, MD, is leading the charge to add vertebral body tethering to the spine surgeon’s toolbox. Dr. Lonner has performed more procedures using the device than any other surgeon worldwide.
In August 2019, vertebral body tethering (VBT) was approved by the U.S. Food and Drug Administration, joining spinal fusion and rigid bracing as time-tested options to treat adolescents with abnormal lateral or side curvature of the spine whose bones have not fully matured. The approval marked an exciting new era in corrective surgery for idiopathic scoliosis and Mount Sinai orthopedic surgeon Baron S. Lonner, MD, is leading the charge to add the procedure to the spine surgeon’s toolbox. Having performed nearly 350 VBT procedures in recent years—more than any other surgeon worldwide with the approved device—Dr. Lonner is well positioned to lead the pack.
Currently, two surgical non-fusion devices have been approved by regulators in the United States. The Tether™ Vertebral Body Tethering System, which was developed by Dr. Lonner and other surgeons as well as a group of engineers, and the ApiFix System (ApiFix Ltd., Israel) for motion-sparing scoliosis correction. Dr. Lonner played an advisory role in the latter device.

“Spinal fusion has performed well traditionally for people with severe spinal deformity, and remains the gold standard,” says Dr. Lonner, who is Chief of Minimally Invasive Scoliosis Surgery and Professor of Orthopedics, and Pediatrics at the Icahn School of Medicine at Mount Sinai. “But if the curvature is moderate and more flexible, then the Tether can deliver excellent outcomes. In fact, we have seen correction of a 50-degree curve down to about 15 degrees or less, for example, while preserving spinal flexibility and function over time. And, patients are able to return to sports and other activities soon after surgery.”
Surgical Differences in the Approved Devices
Dr. Lonner continues to work with industry partners and their engineering and manufacturing arms to nurture the next generation of high-performance, non-fusion technologies and devices for spinal correction. For now, Tether and ApiFix are underscoring the surgical possibilities.
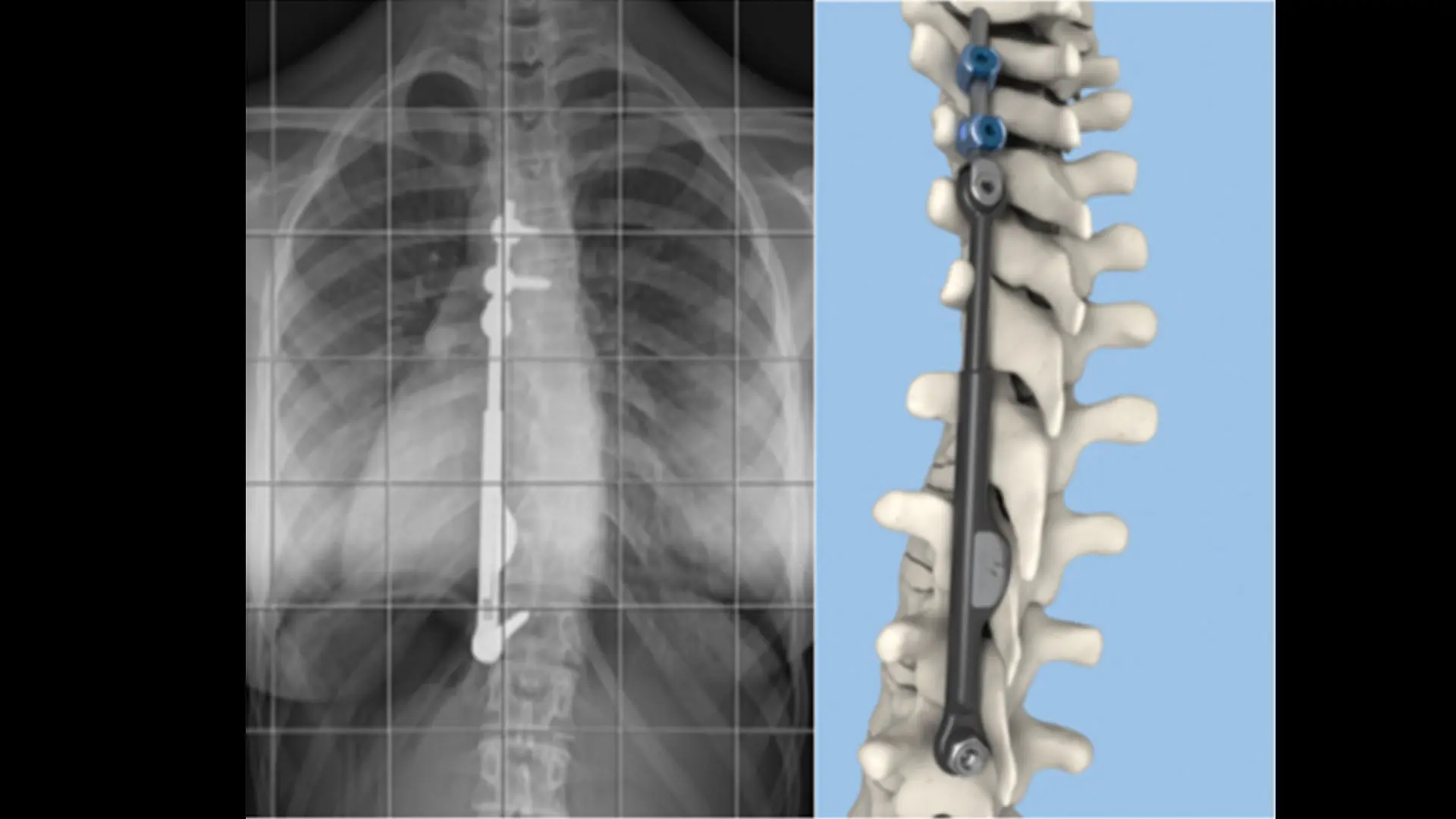
During the Tether procedure, the surgeon places an anchor and bone screws made of a titanium alloy into the patient’s spine on the convex (outwardly curved) side of the spinal curve through an anterior approach. With the help of thoracoscopic visualization and very small incisions, a flexible cord made of a polyethylene-terephthalate polymer is secured to the bone screws, and the surgeon applies tension to the cord to partially straighten the spine. After surgery, the cord continues to straighten the spine while the patient grows.
The ApiFix System is somewhat different, attaching to the spine on the concave side of the curve and maintaining a good deal of the patient’s natural flexibility through a self-adjusting rod mechanism that allows for additional post-operative correction. This procedure is performed from a posterior or back approach. The device can even be removed if the curve remains straight after a corrective period of three or more years. “ApiFix works well for children who have failed with an external brace—either their curve is getting worse or they cannot tolerate it emotionally or psychologically,” notes Dr. Lonner.
The Path Ahead for VBT
Dr. Lonner acknowledges there is a steep learning curve for vertebral body tethering, which might detract from quick and widespread adoption by the orthopedic field. Nonetheless, he has seen a good deal of enthusiasm among colleagues around the world for the now-approved technology, as evidenced by the numbers of surgeons undergoing training to become certified in the use of the technique for their patients. “There will always be a role for fusion surgery because of its ability to address larger curves,” Dr. Lonner allows, “but VBT and ApiFix have shown they can produce dramatic corrections in children with remaining growth. Just as importantly, having these tools available will allow surgeons, together with patients and their families, to be more proactive in addressing spinal curvature earlier on—before it becomes severe and requires fusion correction.”
Concludes Dr. Lonner, “Given the various options I can now offer my patients, this is a truly inspiring time to be a spine surgeon.”
Featured

Baron S. Lonner, MD
Professor Orthopedic Surgery and Pediatrics